


Anatomy and ideal proportion:
A young face is defined by an overall “V” shape given by full cheeks and well-marked cheekbones associated with a well-defined facial oval.
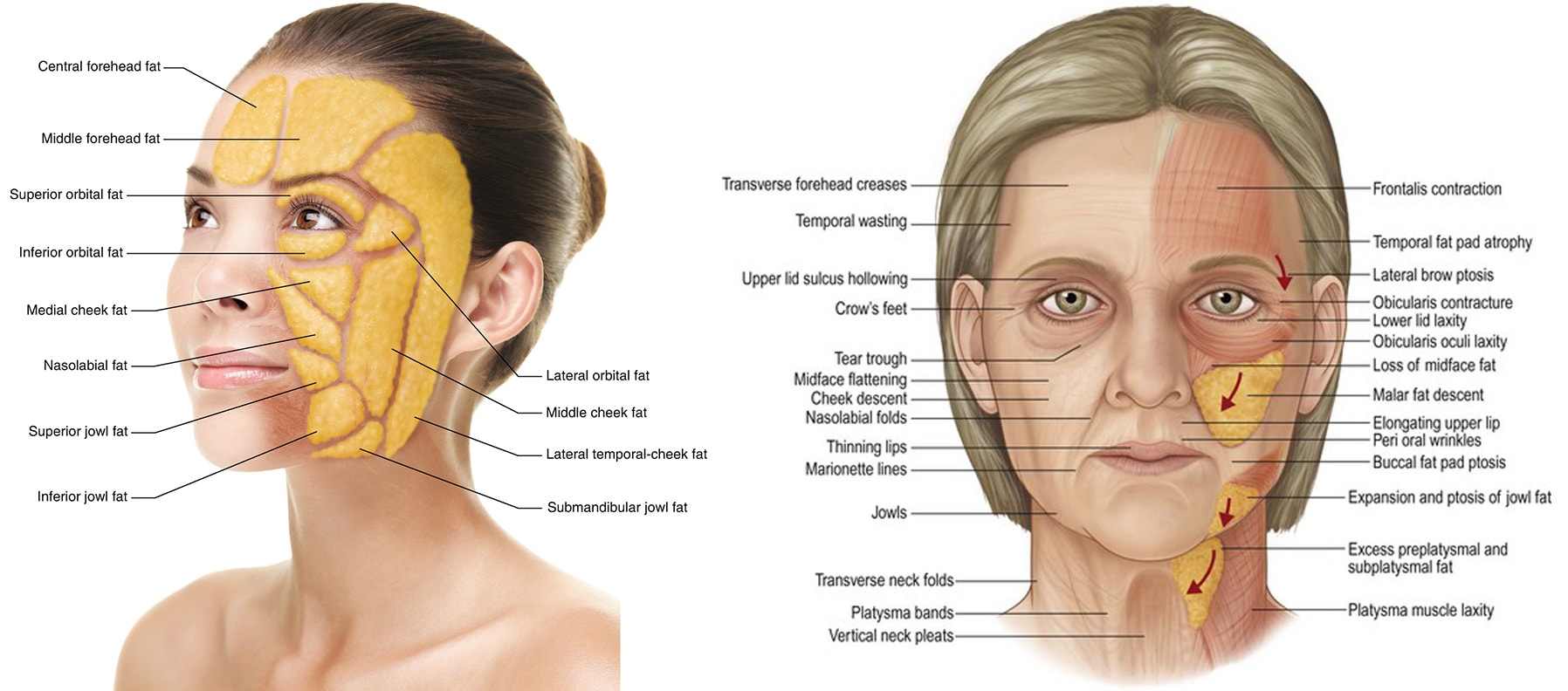
Mechanism of facial aging:
Facial aging is due to sagging of the skin and stretching of the various structural ligaments but also to a relaxation of the musculoaponeurotic system (SMAS). The face sinks downwards with the appearance of nasolabial folds and jowls. This loss of elasticity leading to sagging of the skin is combined with a melting of the various fatty areas of the face over time, which leads to a loss of support.
Surgical lifting, if done properly, does not give a “pulled” appearance but restores the oval of the face that you had 10 – 15 years ago.
Technique:

The facelift can be :s
– supra-SMAS or sub-SMAS (or “deep plane”) depending on the depth of the detachment space
– minilifting or facelift depending on the extent of the detachment
– cervical or facial: a facelift will treat the lower face and the oval of the face while a cervical facelift, with an incision extended backwards at the hairline, will focus on the neck
– with a vertical “restore” component by extending the scar along the hairline to treat the vertical sagging at the cheek and temple.
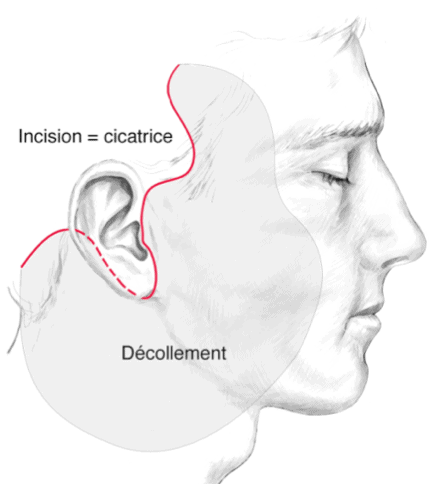
The principle of the surgery is to make an incision around the ear, hidden in the natural folds and shadows around the ear, and to make a space for detachment in order to tighten the structures and resect the excess skin. I perform supra-SMAS lifts where the detachment space is made at a distance from the branches of the facial nerve, because the follow-up is shorter with an identical result and I perform a dual plane with a resection of a SMAS strip and retensioning of the SMAS for severe slackening and associate a vertical component if the clinical examination indicates it. A dual plane procedure gives the same results in absolute terms and in terms of longevity as a “deep plane” facelift with shorter follow-up.
The presence of minimal to moderate sagging combined with minimal to moderate skin excess is a good indication for minilifting.
Facelift or minilift can be combined with fat injections in key support areas to restore volumes lost over time, more superficial fat injections in skin booster and with fractional CO2 laser, to work on texture, fine lines and skin wrinkling.
Results:
Time to final results:
2 weeks to see a significant result, 2 to 5 months to see the final result
Longevity of results :
5 to 10 years for the minilift
8 to 15 years for facelift
Before surgery:
Smoking must be stopped 1 month before the operation (risk of skin necrosis is high if you smoke)
Do not take Aspirin 10 days before the operation, inform Dr. Lucas of any anticoagulant medication (Sintrom, Coumadin, Eliquis, etc.) to arrange for its discontinuation or replacement.
Take Arnica capsules 5 capsules 5 times a day for 5 days before surgery to prevent hematoma.
Intervention :
Pain: the pain during the intervention will be almost non-existent, with an adapted anesthesia
Duration of the procedure: 1h30 for the minilifting / 2h30 for the facelift
Anesthesia: local with sedation for the minilift / general for the facelift
Location: operating room
Outpatient or 1 night hospitalization
After surgery:
Post-operative pain: 1/10 often responding to Dafalgan
Social eviction :
7-10 days with hematoma and swelling
Return to work: 10 days
Return to sport: 3 weeks
Instructions:
Bed rest with no major exertion (which can cause small vessels to open during exertion and result in a hematoma) for 48 hours
Compression bandage around the head for 24-48 hours
Ice for 1 week, as often as possible, to reduce swelling
Arnica capsules 5 capsules 5 times a day for 5 days after surgery to prevent hematoma
Permanent cessation of smoking to prolong the effect of the surgery and minimize complications
Check-up by Dr Lucas on D1, D7, 3 weeks, 3 months, 6 months, 1 year
Sun protection with an index higher than 50 during the 6 months following the surgery.
Follow-up of the scar by Dr. Lucas for 1 year after surgery is essential.
Complications
-A hematoma that may require rapid evacuation.
-A suffering or even a localized cutaneous necrosis, responsible for a delay of cicatrization (the risk is very increased by the tobacco intoxication).
-Infection is exceptional.
Nerve lesions: the lesion of a branch of the facial nerve, likely to lead to paresis, or even facial paralysis, is exceptional and the after-effects usually disappear within a few months.
-Asymmetry
-Deformation of the ear
Abnormal, hypertrophic or even keloid scars, of unpredictable appearance and evolution, can compromise the aesthetic aspect of the result and require specific local treatments. Regular follow-up over time is essential.
Combinations and alternatives
When the sagging (ptosis) and excess skin are too great, surgical lifting is preferable. Non-surgical lifting with threads or hyaluronic acid (the two can also be combined) can be an interesting alternative for patients with moderate ptosis and moderate skin excess, who do not want to have the social eviction that a surgical lifting would have.
The facelift or minilift can be combined with fat injections in key support areas to restore volume lost over time, with more superficial skin booster fat injections, and with the fractional CO2 laser to work on texture, fine lines, and wrinkling of the skin.

















